Blood culture contamination and a potential role for blood culture diversion devices – reflections from HISCON 2026
Blood culture contamination (BCC) has long been recognised as a stubborn and costly challenge in infection prevention and clinical microbiology. At today’s IPC Partners Live session at HISCON 2026 in partnership with Kurin, Phil and I collaborated with Dr Luke Moore and Emily Smith to explore the impact of blood culture contamination and a potential role for blood culture diversion devices in prevention. The session was based on a review article that we have recently published in the Journal of Hospital Infection.
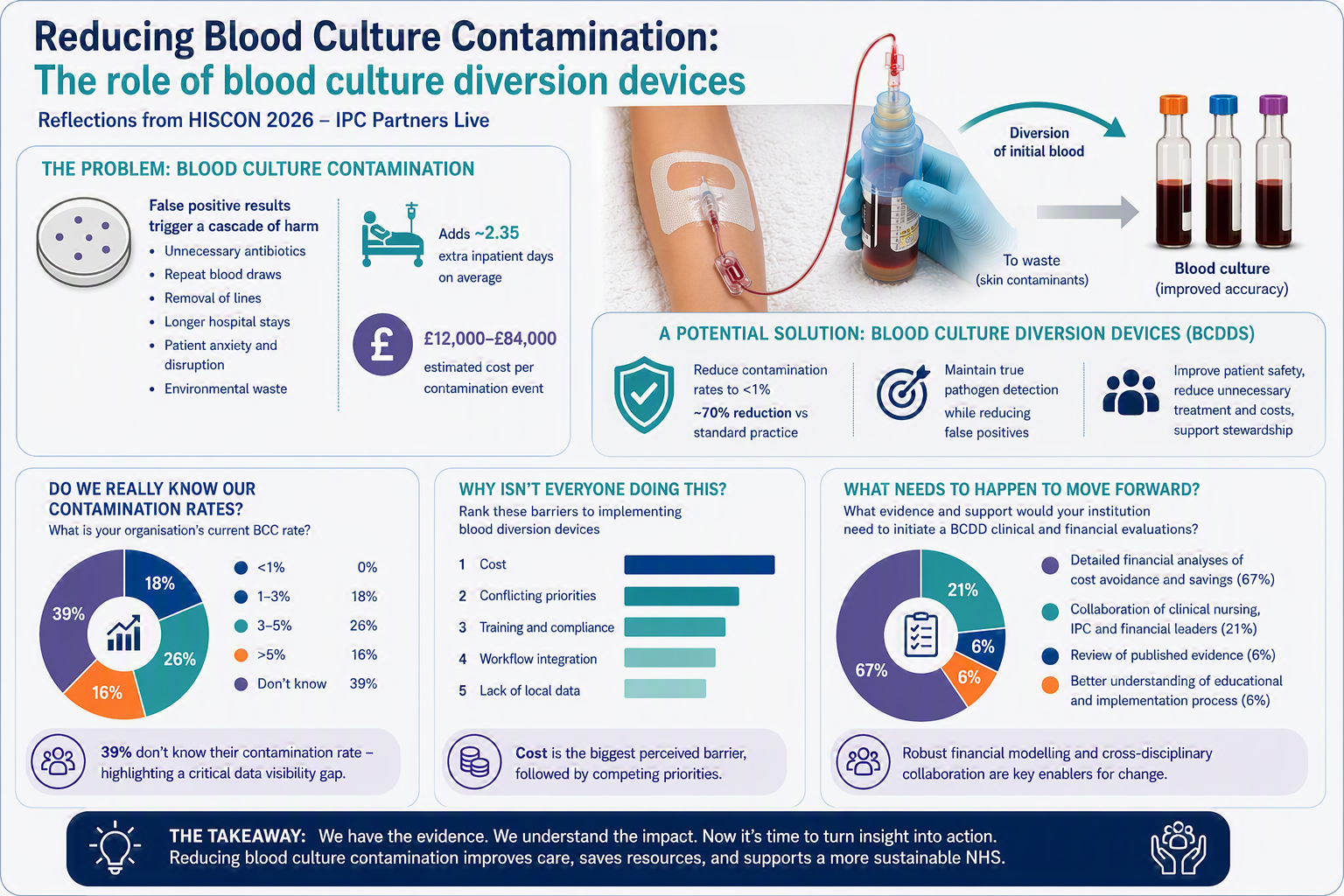
Held at the Royal College of Physicians in London, the session brought together clinical, scientific, nursing, and IPC perspectives to explore the burden of contamination, the evidence for blood culture diversion devices (BCDDs), and the realities of implementing change in pressured healthcare systems.
The lived reality of contamination
We began with a powerful patient-centred perspective from Emily Smith, reminding us that BCC is something that has real impact for patients. BCC can trigger a cascade: repeat venepuncture, unnecessary antimicrobial therapy, removal and reinsertion of vascular access devices, and prolonged uncertainty for patients. These consequences can be difficult to measure and yet are impactful for both patients and from an organizational perspective.
The hidden burden of BCC: clinical, operational, and financial
Dr Luke Moore outlined the broader system impact of BCC. Contamination delays diagnosis, prolongs hospital stays, and drives avoidable antimicrobial exposure. The picture presented reinforced that this is not a marginal issue: BCC adds an additional two inpatient days on average, frequently leads to unnecessary antibiotic use, and contributes to downstream interventions, diagnostics, and environmental waste.
Counting the cost
The financial implications of BCC are difficult to measure but equally striking. Individual contamination events can cost between £12,000 ($16,000) and £84,000 ($111,000). This could add up to millions annually for an organization, much of which is probably avoidable. However, accurately measuring the cost of BCC is difficult, will depend on your perspective, and some of the costs may be "opportunity costs" that don't affect the all-important bottom line / cash balance of an organisation.
BCCDs: part of the solution?
Blood culture diversion devices offer a practical approach to tackling contamination at its source. By diverting the initial portion of a blood draw, where skin contaminants are most likely to be present, these devices can significantly reduce false positive results without compromising true pathogen detection. In doing so, they have the potential to improve diagnostic accuracy, reduce unnecessary antibiotic use and downstream interventions, and support both patient safety and antimicrobial stewardship efforts.
Do we really know our BCC rates?
One of the most revealing aspects of the session came from the live audience polling.
When asked about their organization's current BCC rate:
- 39% said they don’t know
- Only 18% reported rates of 1–3%
- 26% reported 3–5%, and 16% reported >5%
- Notably, no respondents reported rates below 1%
This lack of visibility is telling. Despite BCC being widely discussed, many organisations appear to lack robust or accessible local data. Without this, it becomes difficult to benchmark, build a case for change, or evaluate interventions.
Why isn’t everyone doing this?
Despite some compelling evidence for BCCDs, they are not commonly used. The audience polling provided some useful insight.
Participants ranked barriers to BCCD implementation as follows:
- Cost (ranked the most significant barrier)
- Conflicting priorities
- Training and compliance
- Workflow integration
- Lack of local data
I was not surprised to see cost as the #1 barrier. But I was surprised to see 'lack of local data' considered as the least important. In my view, if you don't have a scaled problem, it's very difficult to secure investment. Otherwise you find yourself seeking investment to solve an invisible problem!
What organisations need to move forward
A final poll explored what would help organisations initiate clinical and financial evaluations of BCDDs.
- 67% identified detailed financial analyses of cost avoidance and savings as the key requirement
- 21% highlighted the need for collaboration across clinical, IPC, and financial leaders
- Only 6% selected published evidence, and 6% implementation/education support
Summary
So where does this leave us? Today’s session reinforced several important points. First, blood culture contamination remains a significant and under-recognised problem, with real consequences for patients, antimicrobial stewardship, and healthcare resources. Second, there is now a strong and growing evidence base for interventions, particularly BCCDs, that can meaningfully reduce contamination. But third, and perhaps most importantly, implementation will require strong cost-effectiveness analysis to demonstrate that the investment in BCCDs is worthwhile.
Subscribe
Subscribe to our email list if you’d like us to let you know about future Journal Clubs, Insight Webinars, and for other updates from IPC Partners.
This website uses cookies to improve your experience. Learn more