It is time to go “water lite”
I visited one of my children’s primary schools recently to talk about Florence Nightingale. One of the things she understood (and something that modern healthcare seems to have largely forgotten) is that the built environment matters. She recognised that light, air, cleanliness – and water – could either support recovery or actively harm patients. More than 160 years later, we find ourselves facing the very real prospect of the post‑antibiotic era, yet there is a tendency among some to overlook one of the most persistent and under‑recognised sources of risk in our hospitals: water and wastewater systems. (Tune in for Dr Jessica Martin’s Insight Webinar on Wednesday this week to hear more about this!)
Water systems: invisible, ubiquitous, and underestimated
Healthcare water systems are complex, extensive, and difficult to control. They intersect with patient care in countless ways: handwash basins, sinks, showers, ice machines, humidifiers, and equipment that uses or discharges water. We know that opportunistic pathogens such as Pseudomonas aeruginosa, Legionella pneumoniae, and non‑tuberculous mycobacteria thrive in these environments.
As resistant organisms have become more prevalent, so too have reports linking outbreaks to sinks and drains. Antimicrobial-resistant organisms are easier to detect and track, but the same pathways have almost certainly been responsible for transmitting susceptible organisms for decades – quietly driving avoidable infections and antibiotic use without ever triggering an “outbreak investigation”.
Why “water‑lite care” entered the conversation
A number of different more-or-less synonomous terms have emerged to describe “water-safe”, “water-lite”, or “water-free” care. The principle change is reducing and restricting the availability of tap water in the clinical environment. So far as the hierarchy of controls goes, this is a sound strategy, with “elimination” of the risk the most fail-safe and desirable from a risk management point of view.
The term “water‑free” is often misunderstood and, actually, not entirely helpful. In most published studies, care was not entirely waterless. Bottled or filtered water was still used for specific tasks such as oral care or medication administration. What changed was where and how water was used.
The most impactful interventions were:
- removal of sinks from patient rooms,
- relocation of handwash stations outside clinical areas,
- elimination of wastewater drainage within the immediate patient environment, and
- substitution of tap water with wipes, pre‑packaged bathing systems, or filtered/bottled water.
Taken together, these measures disrupt all major transmission routes from water and wastewater: splashing, aerosolisation, aspiration, and indirect contact via contaminated surfaces.
So, should we call this strategy “water-free”, “water-safe” or “water-lite”?
- “Water-free”. Well, the problem with this one is that it’s not! Water is necessary for patient care, at least some of the time. One of the unintended consequences of calling the strategy “water-free” is that people remove water sources that are actually necessary for care!
- “Water-safe”. A strong contender. Links directly into the aim of the programme (to improve patient safety). My problem with this one is that you can have a “water-safe” strategy without the removal of any water sources by using ‘traditional’ methods applied rigorously (chemical control, improving flow, water temperature monitoring, water sampling etc).
- “Water-lite”. Despite myself, I am increasingly in favour of this one. A big part of me feels similarly opposed to this term as to how “drive thru” seems to have crept stealthily into the English language!! However, it is the most descriptive of the three, and in the spirit of clear communication with those to whom this idea might be new, I think we should go with it!
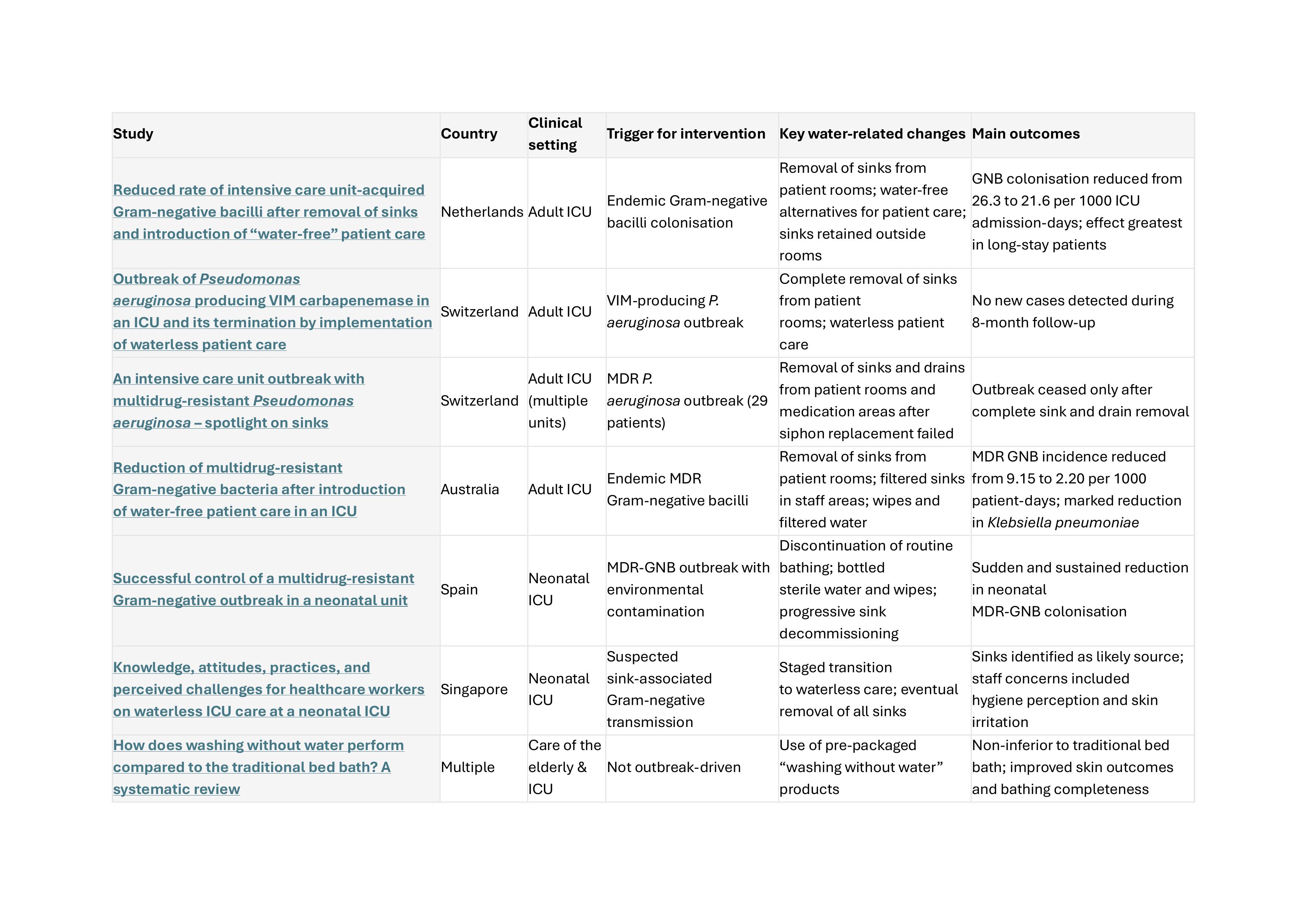
The Journal of Hospital Infection has recently published a narrative review by Inkster et al. summarising the evidence around “water free” care. The move towards water‑lite patient care has typically been driven by crisis. In several intensive care units, particularly during outbreaks involving highly resistant Gram‑negative organisms, conventional infection control measures failed. Only when sinks were removed from patient rooms and water‑based care was replaced with alternatives did transmission stop.
A small but growing body of evidence now shows a consistent pattern: when sinks are removed from patient rooms and patient care is redesigned to minimise water exposure, infections and colonisation with Gram‑negative organisms fall. This has been observed in adult ICUs, neonatal ICUs, and other high‑risk settings, across multiple countries. Crucially, these interventions did not simply eliminate the outbreak strain. They reduced overall acquisition of Gram‑negative organisms, particularly among patients with longer lengths of stay: precisely those at greatest risk from environmental exposure.
Table: Studies evaluating the impact of “water-lite” care in hospitals
Why current approaches are not enough
Surveillance systems lack sensitivity, meaning waterborne transmission events often go unrecognised. Routine water testing and temperature monitoring can provide false assurance: an outlet can test negative today and be contaminated tomorrow, with any resulting infections unlikely to be traced back to the source.
Handwash basins themselves are a double-edged sword. Poor cleaning, inappropriate disposal of fluids, and design flaws can turn them into reservoirs of risk. Observational studies show that sinks are frequently used incorrectly, despite training and policy.
An opportunity to “design out” risk
England is currently undertaking the largest healthcare construction programme in its history. The hospitals being built now will still be in use when AMR is predicted to be at its most severe. Retrofitting solutions later will be expensive, disruptive, and less effective. Designing-out risk at the outset is not only safer, but cheaper.
This does not mean every unit must become fully water‑lite overnight. A spectrum of approaches exists, from removing sinks from patient rooms, to relocating clinical handwash stations, to introducing water‑free bathing. What matters is that water and wastewater risks are properly recognised, assessed, and mitigated.
Just as importantly, staff must be involved. Water‑lite care represents a significant departure from long‑established practice. Concerns about hygiene, patient safety, Clostridioides difficile, skin health, sustainability, and workflow are legitimate and must be addressed through training, evidence, and experience, not dismissed.
Summary
Water‑lite patient care is not a silver bullet, nor is it appropriate everywhere. But the evidence increasingly suggests that continuing to place sinks and drains next to our most vulnerable patients is a risk we can no longer justify. If Florence Nightingale were designing hospitals today, she would almost certainly be asking probing questions about water. And we need to do the same.
Subscribe
Subscribe to our email list if you’d like us to let you know about future Journal Clubs and for other updates from IPC Partners.
This website uses cookies to improve your experience. Learn more