Normothermia: a solved problem that isn't quite solved
There are some patient safety challenges that feel as though they ought to have been solved by now. SSI prevention is one of them! We know what works to reduce the risk of SSI but getting it right every time continues to prove challenging. Surgical prophylaxis is a good example. The number of times we actually achieve the right agent, at the right dose, and at the right timepoint is a lot less common than you might hope! Perioperative hypothermia is another area where we know what to do, but we just aren't great at doing it (or measuring it, for that matter).
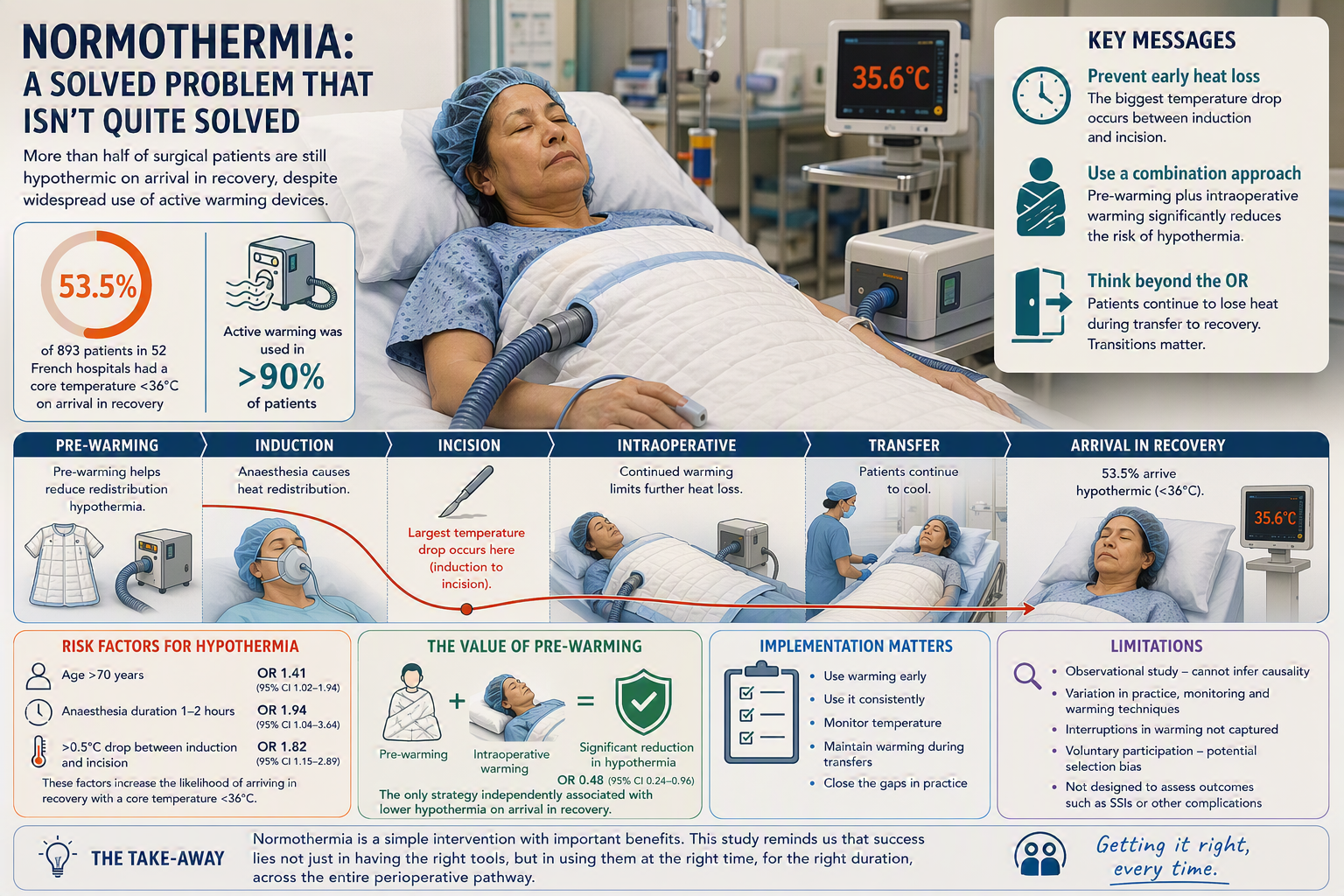
Cue a large French multicentre study published by Alfonsi and colleagues finding that more than half of patients arriving in recovery after surgery remained hypothermic, despite the widespread use of active warming devices.
The challenge isn't equipment
We have a good understanding of the physiology. We have national and international guidance. We have effective warming technologies. And we know that maintaining normothermia is associated with better outcomes for patients, including reduced postoperative complications. And yet in this study of 893 patients from 52 hospitals across France, just more than half (53.5%) of patients had a core temperature below 36°C (i.e. hypothermic) on arrival in recovery. And this is despite active warming having been used in over 90% of patients.
So, if warming technology is being used so widely, why do so many patients remain hypothermic? It's about when and for how long the warming technology was actually applied.
Risk factors for hypothermia
Risk factors for hypothermia included age >70 years (OR = 1.41 [CI95%: 1.02–1.94]), duration of anesthesia from 1 to 2 hours (OR = 1.94 [CI95%: 1.04–3.64]), and a decrease in temperature of >0.5˚C between anesthesia induction and surgical incision (OR = 1.82 [CI95%: 1.15–2.89]). The largest temperature drop occurred between induction of anaesthesia and surgical incision. Patients who experienced a fall in core temperature of more than 0.5°C during this initial phase were almost twice as likely to be hypothermic on arrival in recovery. This supports what we know about the redistribution of heat that occurs during anaesthesia. Once that early temperature loss has occurred, it can be difficult to reverse completely later in the procedure.
The value of pre-warming
The intervention that appeared to make the greatest difference was the combination of pre-warming and intraoperative warming. In the multivariable analysis, this was the only warming strategy associated with a significant reduction in hypothermia on arrival in recovery (OR = 0.48 [CI95%: 0.24–0.96]).
The findings are consistent with previous literature suggesting that pre-warming helps reduce the redistribution hypothermia that occurs during induction of anaesthesia. Pre-warming isn't a magic solution, but that it forms part of an effective pathway that continues throughout the patient's perioperative journey.
Looking beyond the operating theatre
Another observation from the paper was that patients continued to lose heat during transfer from theatre to recovery. Even among patients who received combined pre- and intraoperative warming, temperatures often fell during this transition. This is a useful reminder that we need to think in terms of care pathways rather than care delivered by individual departments. Whether we are thinking about infection prevention, antimicrobial stewardship, deteriorating patients or perioperative care, some of the greatest vulnerabilities occur during transitions. Focusing on a single phase of care may miss important opportunities for improvement elsewhere in the pathway.
Limitations
Several limitations should be considered when interpreting the findings. The study was observational rather than randomised, meaning that associations between warming strategies and outcomes cannot be assumed to be causal. Clinical teams continued their usual practice, introducing potential variation in warming techniques, temperature monitoring, and perioperative care between sites. The limitation around temperature monitoring is an important one, given the variability in performance of various methods to monitor core temperature. The investigators also did not capture periods when warming may have been temporarily interrupted during surgery, which could have affected estimates of warming exposure. In addition, participation was voluntary, raising the possibility of selection bias, and the results may not be fully generalisable beyond the French healthcare setting. Finally, while the study examined hypothermia prevalence, it was not specifically designed to evaluate downstream clinical outcomes such as surgical site infections or other postoperative complications.
A familiar implementation challenge
I was reminded that so many of our healthcare improvement initiatives rely on effective implementation. In this study, the issue wasn't the application of effective technology, but rather effective application of the technology!
Normothermia may not be the most high-profile patient safety issue. It rarely attracts the same attention as antimicrobial resistance, healthcare-associated infection or sepsis. Yet this study reminds us that seemingly routine aspects of care can still present significant opportunities for improvement.
Subscribe
Subscribe to our email list if you’d like us to let you know about future Journal Clubs, Insight Webinars, and for other updates from IPC Partners.
This website uses cookies to improve your experience. Learn more