Tension between IPC risk and sustainability gain: looking for the win‑wins
Infection prevention and control (IPC) and sustainability are often presented as being in tension with one another. From an IPC perspective, the instinctive response to risk is frequently “more”: more PPE, more single-use devices, more cleaning, more isolation. From a sustainability perspective, the same interventions are increasingly recognised as environmentally costly, resource-intensive, and sometimes of marginal benefit. The challenge is that both IPC and sustainability ultimately share the same goal: improving health outcomes, now and in the future. The task for us is to find the scenarios where both sustainability and IPC win (and there are some!).
Why this feels uncomfortable
Many IPC practitioners will be familiar with the frustration of being blamed for anything that is inconvenient, costly, or environmentally unfriendly in healthcare. “Infection control won’t let us…” is a phrase that crops up in relation to everything from flowers on the ward and visitors at Christmas, to washable curtains, food and drink, companion animals, and even Sellotape. In reality, IPC rarely deals in absolutes. Most of our work is risk assessment, proportionality, and sometimes compromise, but this can easily be lost.
At the same time, sustainability teams may see IPC as a barrier to change, particularly when conversations focus on reuse, reduction, or shifting away from single-use products. If framed incorrectly, this can quickly turn into a tug of war: Team IPC versus Team Sustainability. That framing helps no one.
What do we mean by sustainability in healthcare?
The World Health Organization defines a sustainable health system as one that improves, maintains, or restores health while minimising negative impacts on the environment and leveraging opportunities to restore and improve it, to the benefit of current and future generations (WHO, 2017). There are three key elements here that are particularly relevant for IPC:
First, improving health remains non-negotiable. If an intervention really reduces healthcare-associated infections (HCAIs), improves patient outcomes, or saves lives, it is fundamentally aligned with sustainability, even if it has an environmental cost.
Second, we should minimise environmental harm and, where possible, restore. This means questioning whether all current IPC practices deliver meaningful benefit, and whether the same outcome could be achieved in a less resource-intensive way.
Third, sustainability is about benefits now and in the future. Preventing infections today avoids far greater carbon, financial, and human costs tomorrow.
A simple framework: reduce, reuse, replace
Much of the sustainability conversation in IPC can be structured around familiar principles: reduce, reuse, replace (and recycle, where appropriate).
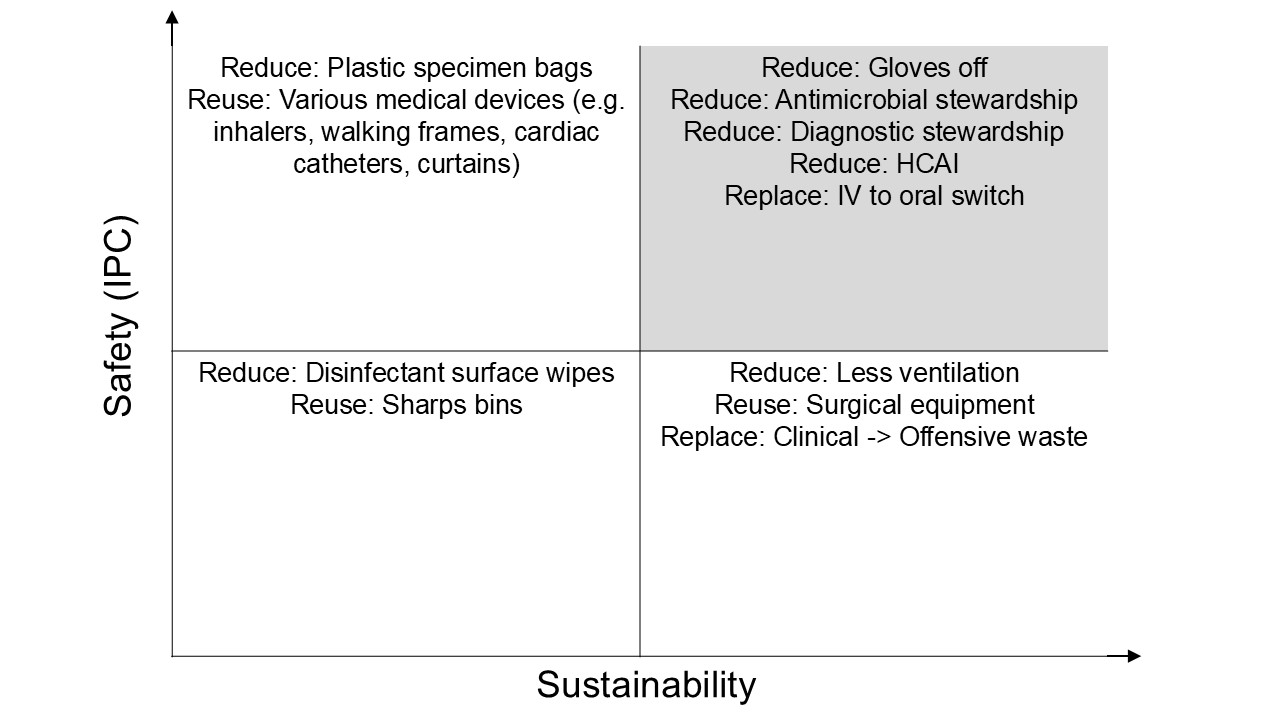
Reduction is often the most powerful lever and frequently aligns well with good IPC. Reducing HCAI is an obvious example: fewer infections mean fewer antibiotics, fewer isolation days, fewer procedures, and fewer consumables. Antimicrobial stewardship and diagnostic stewardship sit firmly in this space. So does challenging unnecessary glove use (“gloves off”), overuse of disinfectant wipes, and excessive ventilation where it is not evidence-based.
Reuse is more uncomfortable for IPC, but not inherently incompatible. Reusable surgical textiles, gowns, drapes, and certain medical devices can be safe when supported by robust decontamination processes. Similarly, rethinking waste streams - such as appropriate reuse or rationalisation of sharps bins and waste containers - can deliver environmental benefits without increasing infection risk, if risk is assessed properly rather than assumed.
Replacement involves changing either products or processes. Examples include switching from intravenous to oral therapy where clinically appropriate, choosing more sustainable PPE products, reclassifying waste from clinical to offensive where safe, or moving away from routine use of disinfectant wipes in favor of “bucket” disinfectant approaches in some scenarios.
The image below illustrates this - we should be looking for win-win initiatives in the "top right" box!
PPE: an uncomfortable case study
The COVID-19 pandemic brought these tensions into sharp focus. PPE use in England increased dramatically between 2019 and 2020, with sustained high volumes thereafter. While PPE undoubtedly played a critical role in protecting healthcare workers, its environmental impact has been stark.
Life cycle analyses of PPE supplied during the pandemic have estimated impacts equivalent to hundreds of disability-adjusted life years lost, measurable harm to ecosystems, and resource depletion costed in the millions of pounds (Rizan et al., J R Soc Med, 2021). This does not argue against PPE, but it does argue strongly against unnecessary PPE use. Good IPC and sustainability are aligned here, with a target of minimal, rational, and safe use of PPE.
Single-use devices and surgery
Single-use medical devices are often seen as the gold standard from an infection risk perspective. By definition, they remove the risk of inadequate decontamination. However, they contribute substantially to healthcare waste and carbon emissions. For example, a typical cataract operation in the UK has been estimated to generate around 182 kg CO₂e, compared with around 6 kg CO₂e for the same procedure in India (Bhutta, Ann R Coll Surg Engl, 2021). Some of this difference reflects broader system factors, but single-use culture plays a role.
Importantly, emerging evidence suggests that hybrid or reusable surgical instruments can significantly reduce environmental impact and overall cost without increasing infection risk, when managed properly (Rizan & Bhutta, Surg Endosc, 2022). This challenges the old idea that “single use equals safer” in all contexts.
Antimicrobials and environmental harm
Antibiotics are essential to modern healthcare, but they are also environmental pollutants. In addition to the carbon footprint associated with drug manufacture and disposal, antibiotics exert selective pressure in the environment. One well-known example described extraordinarily high concentrations of ciprofloxacin in wastewater from pharmaceutical manufacturing, exceeding therapeutic levels in humans and exceeding total national daily consumption in some countries (Carlsson et al., Environ Toxicol Chem, 2009).
This strengthens the case for antimicrobial stewardship. Using fewer antibiotics, using them more precisely, and shortening durations where safe all reduce environmental harm while improving patient care.
IV to oral switch: a clear win‑win
Switching from intravenous to oral therapy, where clinically appropriate, is one of the clearest examples of alignment between IPC, patient safety, sustainability, and cost. Intravenous therapy carries risks, including extended inpatient stay, line-related infection and phlebitis. It is also far more carbon-intensive. For paracetamol, oral administration has been estimated to have a carbon footprint dozens of times lower than intravenous formulations (Elii et al., BMJ, 2023). Quality improvement projects focused on avoiding unnecessary cannulation have delivered substantial financial savings alongside carbon reductions.
What can IPC practitioners do?
This agenda can feel overwhelming, but individual IPC practitioners can make a difference. Measuring the carbon footprint of infection, engaging with Trust sustainability teams, understanding local sustainability strategies, and starting small, well-defined projects can all help shift the conversation from conflict to collaboration.
Perhaps most importantly, IPC professionals need to be at the table, not perceived as blockers but as partners. Our expertise in risk assessment, systems thinking, and unintended consequences is exactly what is needed to ensure sustainability initiatives genuinely improve health rather than simply shifting risk elsewhere.
This isn’t about IPC vs. sustainability. The challenge is recognising that good IPC is fully aligned with sustainable healthcare, and that poor, wasteful, ineffective IPC practice is not.
Subscribe
Subscribe to our email list if you’d like us to let you know about future Journal Clubs, Insight Webinars, and for other updates from IPC Partners.
This website uses cookies to improve your experience. Learn more