Big Data and AI – the future of IPC
Over the past decade, IPC has begun a quiet but significant transformation. We have always worked with data: surveillance reports, laboratory results, audit findings. But the scale, speed, and complexity of the data now available to us is fundamentally different. Electronic health records, real-time microbiology feeds, and system-wide surveillance platforms generate volumes of information that far exceed what traditional approaches can realistically process. If we continue to apply “old” methodology we will miss out on huge potential benefits.
This is why there is so much interest in big data and artificial intelligence (AI). These technologies offer the potential to turn fragmented, complex data into meaningful insights that can inform frontline decision-making. As IPC professionals, we are increasingly being asked to engage with these tools and to lead on how they are implemented in practice.
Next Wednesday, Dr Nneoma Okeke will lead an Insight Webinar exploring how big data and AI are beginning to reshape IPC, which I can’t wait for! Many of us are still at the early stages of this journey, trying to understand what these technologies can (and cannot) deliver in real-world healthcare settings.
The ways in which big data and AI can support IPC
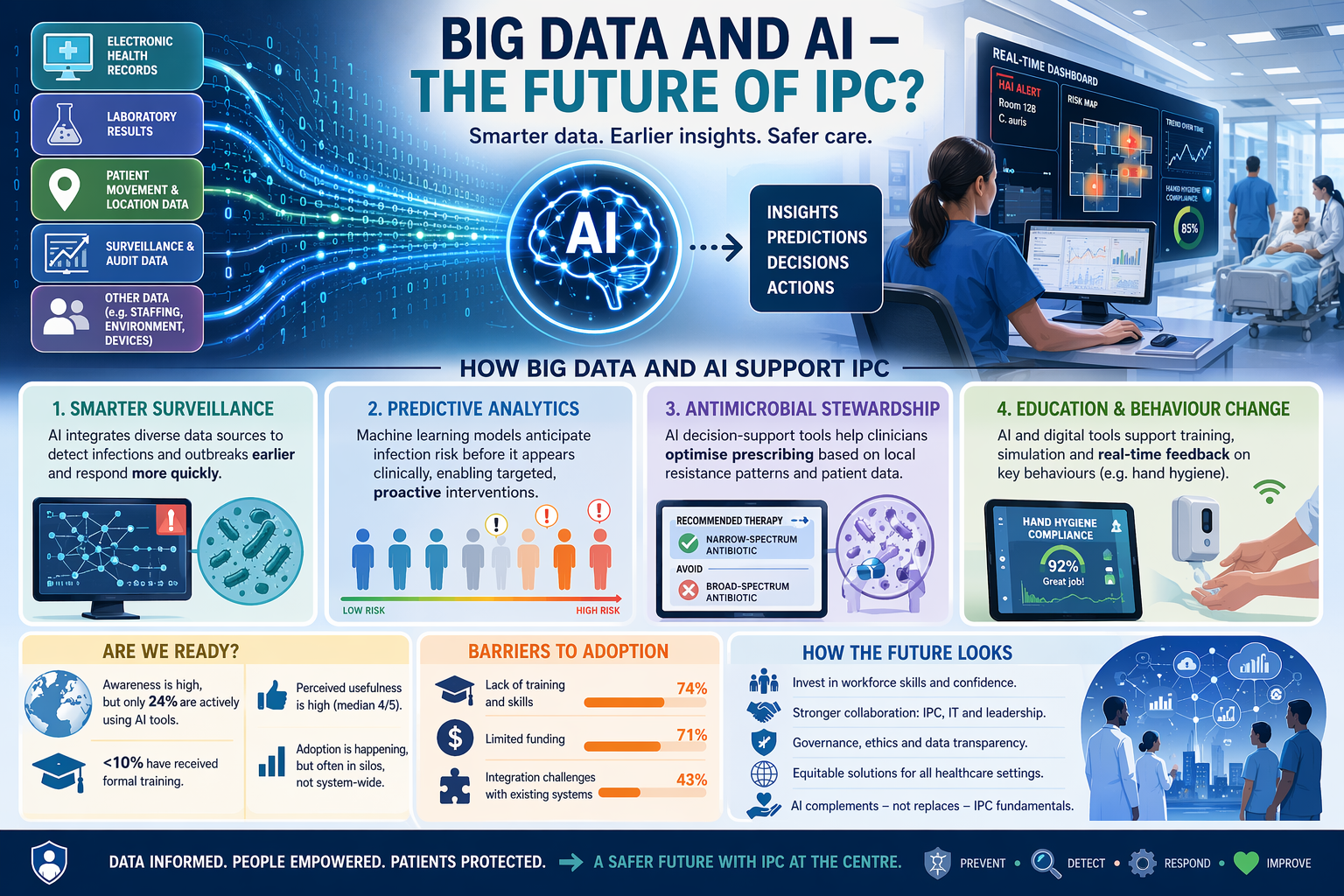
The value of big data and AI in IPC lies in their ability to synthesise complex datasets and identify patterns that would otherwise go unnoticed. This is particularly important in an environment where infections emerge dynamically and often unpredictably.
- One of the clearest applications is in surveillance. AI-driven systems can integrate electronic health record data, laboratory results, and patient movement information to support earlier detection of healthcare-associated infections and outbreaks, enabling a more timely response.
- There is also growing interest in predictive analytics - using machine learning models to anticipate infection risks before they appear clinically. This moves IPC from a reactive to a more proactive footing, allowing interventions to be dynamically targeted at patients or settings where risk is highest.
- These technologies are beginning to support antimicrobial stewardship through decision-support systems, helping clinicians optimise prescribing based on complex and evolving resistance patterns.
- AI and digital tools are also increasingly being used to support education and training, from simulation platforms to real-time feedback on compliance with key behaviours such as hand hygiene.
Are we ready?
I was interested to read a recent paper by Gastaldi and colleagues providing a timely and important global perspective on where we currently stand. It is based on a WHO survey of 441 IPC professionals across all six WHO regions, offering one of the most comprehensive snapshots to date of AI adoption in our field.
Perhaps the most important finding is the gap between awareness and implementation. While most respondents reported some familiarity with AI and digital technologies, only around a quarter were actively using them in practice, and fewer than one in ten had received formal training.
Among those already using AI, the applications were diverse but relatively focused. The most common uses included AI-based analysis for research, semi-automated surveillance systems, AI-supported teaching tools, and antimicrobial resistance detection tools. This suggests that adoption is happening, but often in specific areas rather than as part of a coordinated, system-wide strategy.
Encouragingly, perceptions of usefulness were generally positive. Across a range of IPC tasks including real-time surveillance, outbreak prediction, antimicrobial resistance monitoring, and staff training respondents rated AI and digital tools favourably, typically with median usefulness scores of 4 out of 5. However, these perceptions were not uniform, reflecting differences in local context, digital maturity, and access to resources.
The barriers to adoption included workforce capacity, funding, and system integration. Lack of training and skills was the most commonly cited barrier (74%), followed closely by limited funding (71%) and challenges integrating new tools with existing systems (43%).
Taken together, these findings point to a field that recognises the potential of AI but hasn’t yet fully integrate it into routine practice. I can fully relate to this position. In my own hospitals, we are just beginning to explore the possibilities offered by AI, and have already implemented a few AI-based tools. But there is much more to come.
How the future looks
Looking ahead, it is clear that AI and big data will become increasingly embedded within IPC. I suspect things will look very different in 10 years time, with big data and AI integral to what we do. We need to ensure that this transition happens in a way that is safe, equitable, and genuinely improves patient outcomes.
The WHO survey highlights that progress will depend more on implementation capability than on technological innovation. And so we need to invest in workforce development so that IPC teams have the skills and confidence to work with these tools. This will require stronger collaboration between IPC, IT, and organisational leadership to ensure that systems are interoperable and aligned with clinical workflows. And we need to keep an eye on the development of governance frameworks that address questions of transparency, accountability, and data ethics.
Many AI solutions are developed in and for high-resource settings, but their benefits need to extend across all healthcare contexts. This will require adaptation, co-design, and sustained investment in digital infrastructure, particularly in lower-resource environments.
There is a risk that a focus on digital innovation will detract from the hands-on fundamentals of IPC. AI must not be seen as a replacement for clinical judgement, experience, or basic infection prevention measures.
I’m really excited to be part of the transition to a much more effectively digitally-informed IPC world, and if we get this right, it will help us to protect patients and staff from preventable harm.
Subscribe
Subscribe to our email list if you’d like us to let you know about future Journal Clubs, Insight Webinars, and for other updates from IPC Partners.
This website uses cookies to improve your experience. Learn more